Overview
| Panel | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
|
(Click an image below to enlarge.)
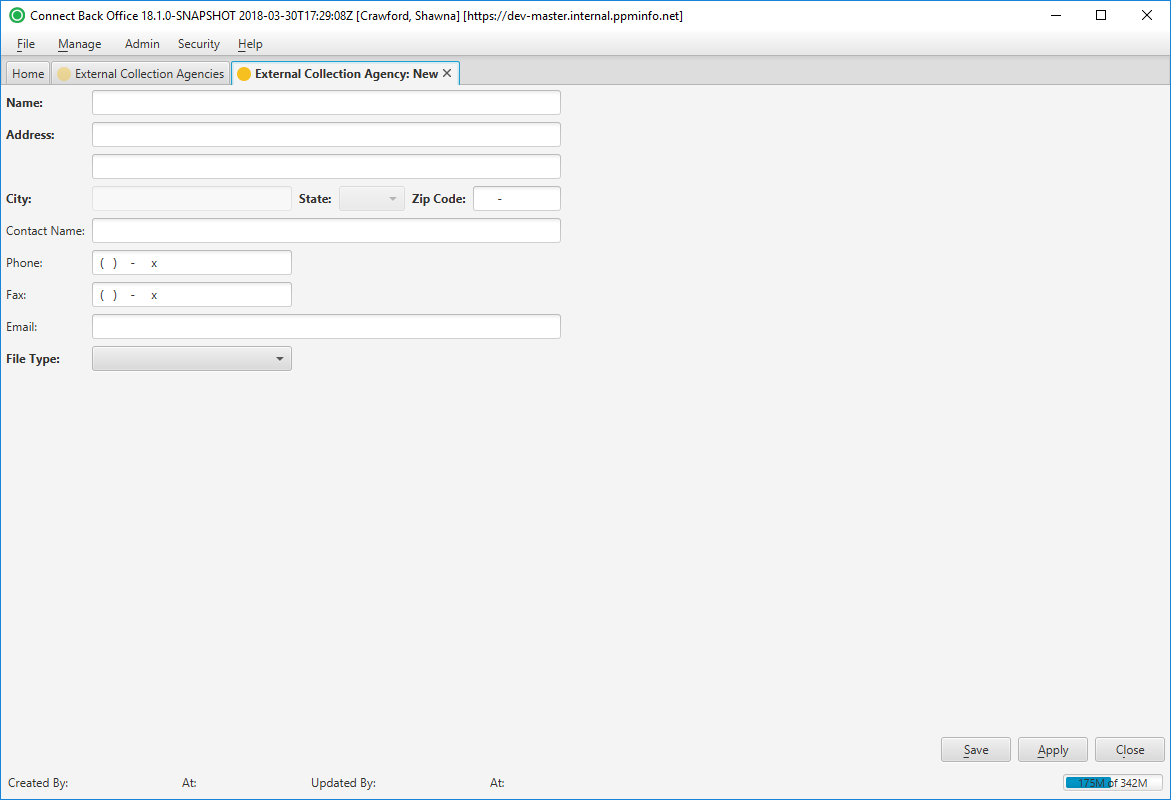
External Collection Agency: New Page
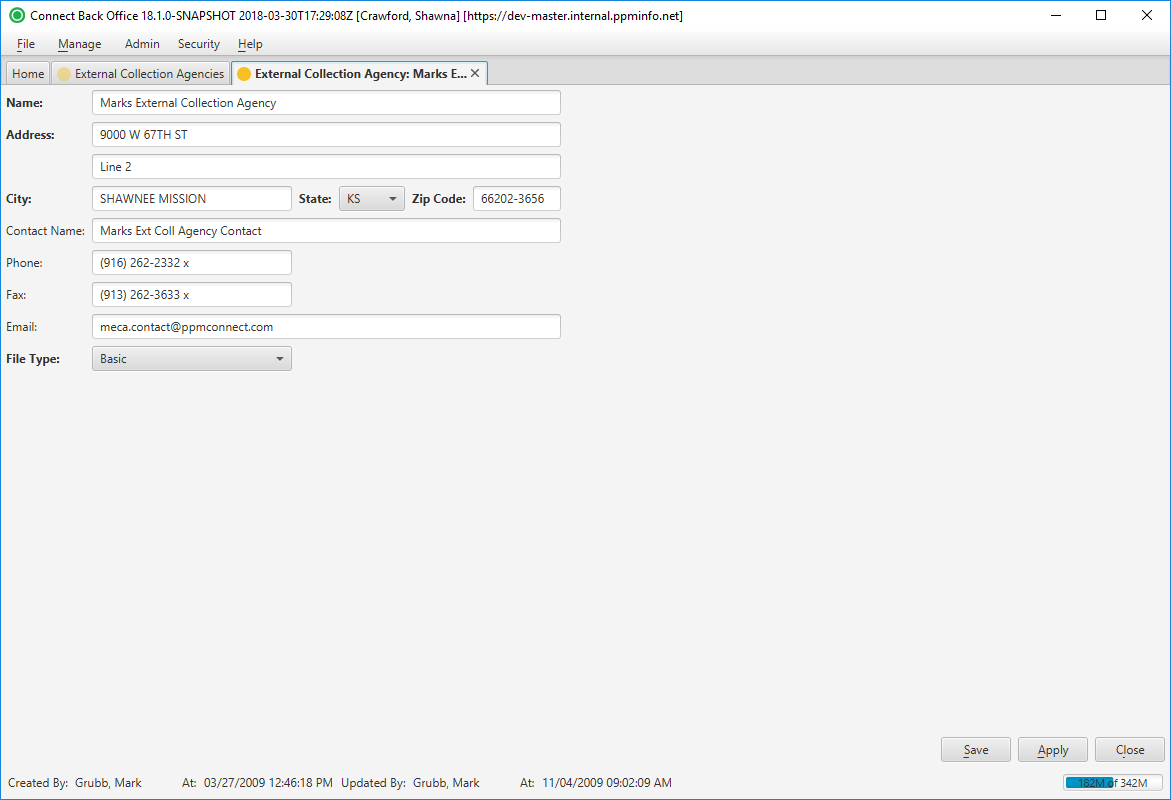
External Collection Agency: [name] Page
Field Definitions
Field | Type | Required | Description |
|---|---|---|---|
| Name | Free Text | Yes | The name of the external collection agency. This information must be unique. |
| Address | Free Text | Yes | The street address (lines 1 and 2) of the external collection agency. |
| City | Free Text | Yes | The city where the external collection agency is located. The field will auto-populate when the Zip Code is entered. However, the field can be edited by typing the name of the city in the space provided. |
| State | Drop Down | Yes | The two-character state abbreviation of the external collection agency address. The field will auto-populate when the Zip Code is entered. However, the field can be edited by typing the state abbreviation or selecting an option from the drop down list. |
| Zip Code | Free Text | Yes | The five-digit plus 4-digit postal code where the external collection agency is located. |
| Contact Name | Free Text | No | The person who is the primary contact at the external collection agency. |
| Phone Number | Free Text (Numeric) | No | The 10-digit telephone number and extension, if applicable, of the external collection agency. |
| Fax Number | Free Text (Numeric) | No | The 10-digit telephone number and extension, if applicable, of the fax machine at the external collection agency. |
| Free Text | No | The electronic mail address of the contact at the external collection agency. | |
| File Type | Drop Down | Yes | The file format used for outputting the external collections file to the to the external collection agency. The file type determines which fields are fields are included in the output file, and can be either Basic, Extended or Full CSV or XML. |
The following table includes the list of fields for the specified file type. The Basic and Extended file type is a CSV (spreadsheet) file. The Full file type is an XML file.
| CSV | XML | Basic (field included) | Extended (fields included) | Full |
|---|---|---|---|---|
Account ID Date of Service Procedure Billed Amount Adjustments Contractual Write-Offs Payments Balance Transferred to ExCol Last Statement DateBalance Guarantor Name Guarantor SSN Guarantor DOB Guarantor Address Guarantor City Guarantor State Guarantor Zip Code Guarantor Daytime Phone Patient Name Guarantor Evening Phone Guarantor Patient SSN Patient DOB Account ID Date of Service Procedure Balance Guarantor NameGuarantor DOB Guarantor Employer Guarantor SSN Guarantor DOB Patient Name Primary Insurance Guarantor Address Guarantor Primary Insurance City Guarantor Primary Insurance State Guarantor Primary Insurance Zip Code Guarantor Patient Daytime Phone Guarantor Patient Evening Phone Patient DOB Patient NameSSN Patient Employer Patient Daytime Phone Procedure Facility Rendering Provider Referring ProviderPatient Evening Phone Primary Insurance Name Primary Insurance Address Primary Insurance City Primary Insurance State Primary Insurance Zip Code Primary Insurance Member IDSubscriber Name Primary Insurance Group IDSubscriber DOB Primary Insurance Subscriber Group ID Primary Insurance Subscriber NameMember ID Primary Insurance Subscriber DOBID Secondary Insurance Name Secondary Insurance Address Secondary Insurance City Secondary Insurance State Secondary Insurance Zip Code Secondary Insurance Member IDSubscriber Name Secondary Insurance Group IDSubscriber DOB Secondary Insurance Subscriber Member ID Secondary Insurance Subscriber NameGroup ID Secondary Insurance Subscriber DOBID Tertiary Insurance Name Tertiary Insurance Address Tertiary Insurance City Tertiary Insurance State Tertiary Insurance Zip Code Tertiary Insurance Subscriber Name Tertiary Insurance Member IDSubscriber DOB Tertiary Insurance Group ID Tertiary Insurance Subscriber Member ID Tertiary Insurance Subscriber NameTertiary Insurance Subscriber DOBID Payment Plan Start Date Payment Plan Payment Plan Amount Payment Plan Due Day of Month Payment Plan Interval Days | Account Number Payment Plan Start Date Payment Plan Indicator Returned Mail Status Indicator Guarantor First Name Guarantor Middle Name Guarantor Last Name Guarantor Suffix Guarantor Gender Guarantor Marital Status Guarantor Language Guarantor SSN Guarantor Date of Birth Guarantor Date of Death Guarantor Daytime Phone Guarantor Evening Phone Guarantor Email Guarantor Employment Guarantor Occupation Guarantor Address Guarantor Address History Account Notes Procedure Name Procedure Code Date of Service Facility Billed Amount Balance Facility Financial Class Patient Name Patient Gender Guarantor Marital Status Guarantor Language Patient SSN Patient Date of Birth Patient Date of Death Patient Daytime Phone Patient Evening Phone Patient Email Patient Employment Patient Occupation Patient Address Patient Address History Rendering Provider Referring Provider Primary Insurance Name Primary Insurance Payer Primary Insurance Rank Primary Insurance Address Primary Insurance City Primary Insurance State Primary Insurance Zip Code Primary Insurance Member ID Primary Insurance Group ID Primary Insurance Subscriber ID Primary Insurance Subscriber Name Primary Insurance Subscriber DOB Primary Insurance Subscriber SSN Secondary Insurance Name Secondary Insurance Payer Secondary Insurance Rank Secondary Insurance Address Secondary Insurance City Secondary Insurance State Secondary Insurance Zip Code Secondary Insurance Member ID Secondary Insurance Group ID Secondary Insurance Subscriber ID Secondary Insurance Subscriber Name Secondary Insurance Subscriber DOB Secondary Insurance Subscriber SSN Tertiary Insurance Name Tertiary Insurance Payer Tertiary Insurance Rank Tertiary Insurance Address Tertiary Insurance City Tertiary Insurance State Tertiary Insurance Zip Code Tertiary Insurance Member ID Tertiary Insurance Group ID Tertiary Insurance Subscriber ID Tertiary Insurance Subscriber Name Tertiary Insurance Subscriber DOB Tertiary Insurance Subscriber SSN Claim TypType Payments Adjustments |